Data User Guide | Exploration
In the exploration phase, you gain an initial overview of the health data landscape and position your own data-driven innovation idea within it. At this stage, you focus on understanding which types of data exist, where they are located and what kinds of use are generally possible.
Even if you already have a concrete idea in mind, exploring the available data remains an important step. By examining existing data sources, you may discover alternative perspectives, identify data that better fit your intended purpose or uncover new directions that you had not considered before.
This exploration creates the foundation for the following phases. When you understand the data landscape well, you can assess later ideas more realistically and develop them in a more targeted way.
Secondary use of health data
Health data emerge in many different contexts. You encounter them during the provision of care, in billing and administrative systems, in clinical registries or as part of scientific studies. In practice, you can engage with health data in different ways. You can reuse existing data, either from your own organization or from external data holders, or you can generate new data through your own studies or interventions.
When you reuse existing data, you apply data that were originally collected for another purpose to answer new questions. This may involve datasets that already exist within your organization or data that you obtain from external sources. If existing data do not sufficiently address your question, you can also generate new data through interventional or non-interventional studies.
In practice, you often combine these approaches. The secondary use of existing data plays a particularly important role for research and innovation because it allows you to analyze relationships, observe developments over time and support decisions with a broader empirical basis without the need for extensive new data collection (Kilgus et al., 2024). By reusing available data, you can generate new knowledge while using resources within the health system more efficiently.
Data types and illustrative use cases
Health data exists in different forms, each of which is suitable for different types of applications. For a basic understanding, it is helpful to distinguish between central data categories, even though overlaps frequently occur in practice (European Commission, 2025; Otto, 2011). The following structure therefore serves as an orientation rather than a strict classification.
Clinical routine data
Is generated during the delivery of care. It includes information on diagnoses, treatments, and clinical courses and are particularly well suited for analyzing care pathways, identifying treatment patterns, or assessing aspects of quality of care. Electronic health records and clinical information systems represent typical sources for this type of data (Hersh et al., 2013; European Commission, 2025).
Care and claims data
Provides insights into delivered services and their reimbursement. It is often used to analyze care structures, identify regional differences, or examine health economic questions. Due to their broad population coverage, it is especially relevant for large-scale and population-based analyses (Busse et al., 2017).
Registry data
Systematically capture specific conditions, interventions, or events over extended periods of time. It enables long-term observations, outcome analyses, and the study of rare diseases. Because of their structured design, registry data support comparative analyses and the observation of trends over many years (Gliklich et al., 2020).
Research data
Is generated in the context of scientific studies or projects. This includes data from interventional and non-interventional studies, observational research, or methodological projects. Beyond primary analysis, these datasets are frequently reused for secondary analyses or for the development of analytical methods (Creswell & Creswell, 2018).
Person-generated health data
Increasingly emerges outside traditional care settings, for example through wearables, mobile applications, or patient-reported outcomes. This data provides insights into everyday behavior, continuous health trajectories, and subjective experiences, thereby complementing established clinical data sources (Sharon, 2017; European Commission, 2025).
Imaging and sensor data
Includes radiological images, monitoring data from medical devices, or continuously collected measurements from sensors. Due to its volume and technical characteristics, it often differs significantly from structured routine data in terms of storage, processing, and analysis requirements (Kahn et al., 2016).
Public health and contextual data
Originates from statistical sources, environmental monitoring, or open data platforms. It is frequently used to situate clinical data within a broader societal or regional context, for example in public health analyses (WHO, 2021).
Taken together, these examples illustrate that different data types have distinct strengths and usage potentials. The exploration phase supports organizations in recognizing these potentials at an early stage and situating them meaningfully in relation to their own objectives.
Situating exploration within the European Health Data Space
Within the exploration phase, the EHDS acts as an important regulatory context that shapes how you approach the health data landscape. At this stage, you do not analyze the regulation in detail. Instead, you consider how the EHDS influences data availability, access pathways and the conditions under which health data can be used in Europe.
If you want to access health data in Europe, you should take into account that personal health data for secondary use will typically be processed within a secure processing environment (Art. 73 et seq. EHDS Regulation) and under clearly defined access conditions. When you explore potential data sources or develop early use case ideas, these structural conditions influence which options appear realistic.
The goal of this phase is therefore not to interpret legal provisions. Instead, you examine how the EHDS shapes where relevant data may exist, how access may be organized and which types of data use appear feasible. This helps you assess potential data sources more realistically and align early ideas with the emerging European health data ecosystem.
By considering the EHDS context during exploration, you can better judge which ideas appear plausible, which data sources may support your initiative and how your early assumptions fit within the evolving European health data environment. This allows you to identify both opportunities and constraints before moving into more detailed concept development.
Key Roles in the European Health Data Space
| Term / Role | Short Definition | Relevant Article |
| Health Data Access Body (HDAB) | National authority responsible for organising access to electronic health data for secondary use, assessing applications and issuing decisions | Art. 55, Art. 57 |
| Union health data access service | EU-level coordination and contact point supporting cross-border access to health data for secondary use |
Art. 56 |
| Health Data Holder | Actor that falls under the EHDS obligations to make certain categories of electronic health data available. The definition is provided in Art. 2(2), while the obligations to make data available are defined in Art. 50 and Art. 51 | Art. 2(2), Art. 50, Art. 51 |
| Trusted Health Data Holder | A Health Data Holder designated by a Member State for which a simplified procedure may apply. It may assess applications and provide data through a secure environment, while the final decision remains with the HDAB | Art. 72 |
| Health Data User | Natural or legal person intending to use electronic health data for permitted secondary use purposes. This role emerges from the provisions governing applications and user obligations | Art. 61, Art. 67 |
| Health data access application | Formal application requesting access to electronic health data for secondary use | Art. 67 |
| Data permit | Official decision authorising access to electronic health data for a specified secondary use purpose | Art. 68 |
| Health data request | Request for data access or analytical results through an alternative procedural pathway to the standard data permit process | Art. 69 |
| Secure Processing Environment (SPE) | Secure technical infrastructure where electronic health data are processed for secondary use under strict security and data protection safeguards | Art. 73 |
| HealthData@EU | Cross-border infrastructure enabling access to electronic health data for secondary use across EU Member States | Art. 75 |
| Dataset description / dataset catalogue | Structured descriptions of available datasets published in catalogues to make data discoverable | Art. 77 |
| Minimum categories of electronic health data for secondary use | Categories of electronic health data that Health Data Holders must make available for secondary use | Art. 51 |
| Purposes for secondary use | Permitted purposes for which electronic health data may be used under the EHDS | Art. 53 |
| Prohibited secondary use | Types of data use that are explicitly prohibited under the EHDS | Art. 54 |
| Right to opt out | Right of individuals to object to the processing of their personal electronic health data for secondary use | Art. 71 |
| Health data intermediation entity | Entity that may support Health Data Holders by facilitating the management of access procedures and data sharing processes | Related to provisions on data holder obligations in the secondary use framework |
Access pathways for secondary use of health data
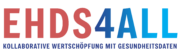
Within the EHDS, access to health data for secondary use can take place through different pathways that reflect distinct governance logics and organizational arrangements. These access routes illustrate how data may be made available in practice while ensuring that legal, organizational and technical safeguards are respected. Across all pathways, datasets are generally expected to be prepared in anonymized or pseudonymized form in accordance with both the EHDS Regulation and the General Data Protection Regulation. Independent of the specific route chosen, the analysis of personal health data is typically required to take place within a secure processing environment (Art. 73 et seq. EHDS Regulation), ensuring that access remains controlled and purpose-bound.
Public access pathway via Health Data Access Body
The primary pathway foreseen by the EHDS follows a publicly governed access model and takes place via a Health Data Access Body. To use this pathway, you have to submit a formal application that describes the intended purpose of use, the requested datasets and the planned safeguards. The Health Data Access Body evaluates the request, coordinates with relevant data holders and oversees the preparation of the dataset, including anonymization or pseudonymization where necessary. The institutional responsibilities and procedural duties of Health Data Access Bodies are defined in Art. 57 et seq. EHDS Regulation, outlining their role in assessing applications, ensuring compliance with legal requirements and facilitating secure data provision.
Once approval is granted, you can access the requested data within a secure processing environment. From your perspective, this pathway provides a comparatively high level of legal certainty and does not require direct negotiation with individual data holders, although the application process may involve preparation effort and defined review timelines.
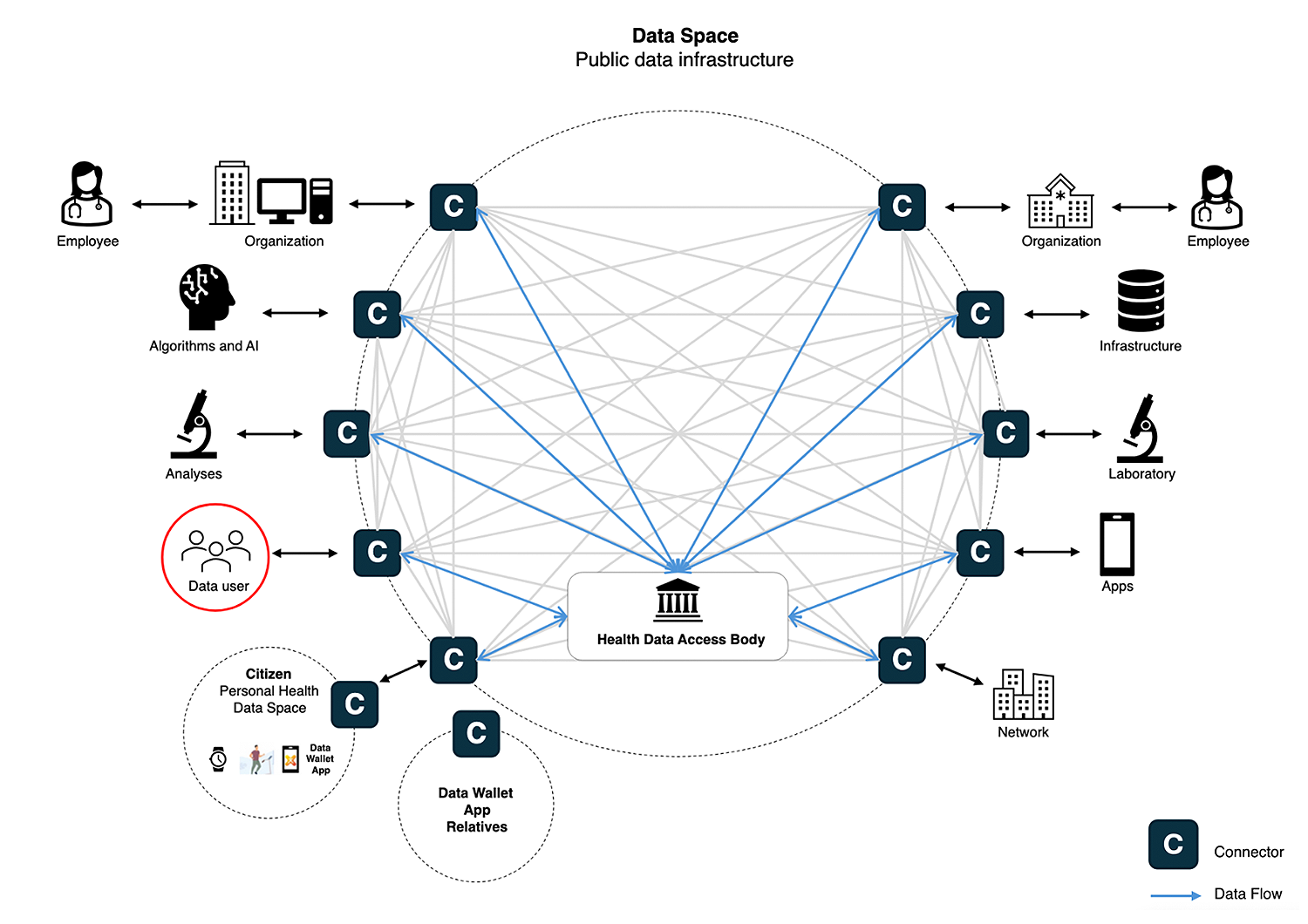
Getting individual consent from data owner
A second pathway relies on the explicit consent of individuals whose data you want to use. In this case, consent serves as the primary legal basis under the GDPR (Art. 6(1)(a) and Art. 9(2)(a)), while the EHDS provides the broader governance context for how such data may be reused.
In practice, you typically collaborate with a data-holding organization that manages the consent process, prepares the dataset and ensures that the agreed purpose of use is respected. The EHDS also strengthens individuals’ rights regarding their own health data. Individuals may request that their personal health data be transmitted to another party, and data holders must enable such transfers within defined timeframes and without charging the individual. This can facilitate consent-based data reuse scenarios, for example when individuals actively agree to share their data for specific research purposes.
Even when consent serves as the legal basis, you should expect that datasets undergo anonymization or pseudonymization before analysis and that you process them within a secure processing environment. For you as a data user, this pathway can offer flexibility for specific research projects or targeted studies. At the same time, it requires careful organizational coordination and clearly documented consent procedures.
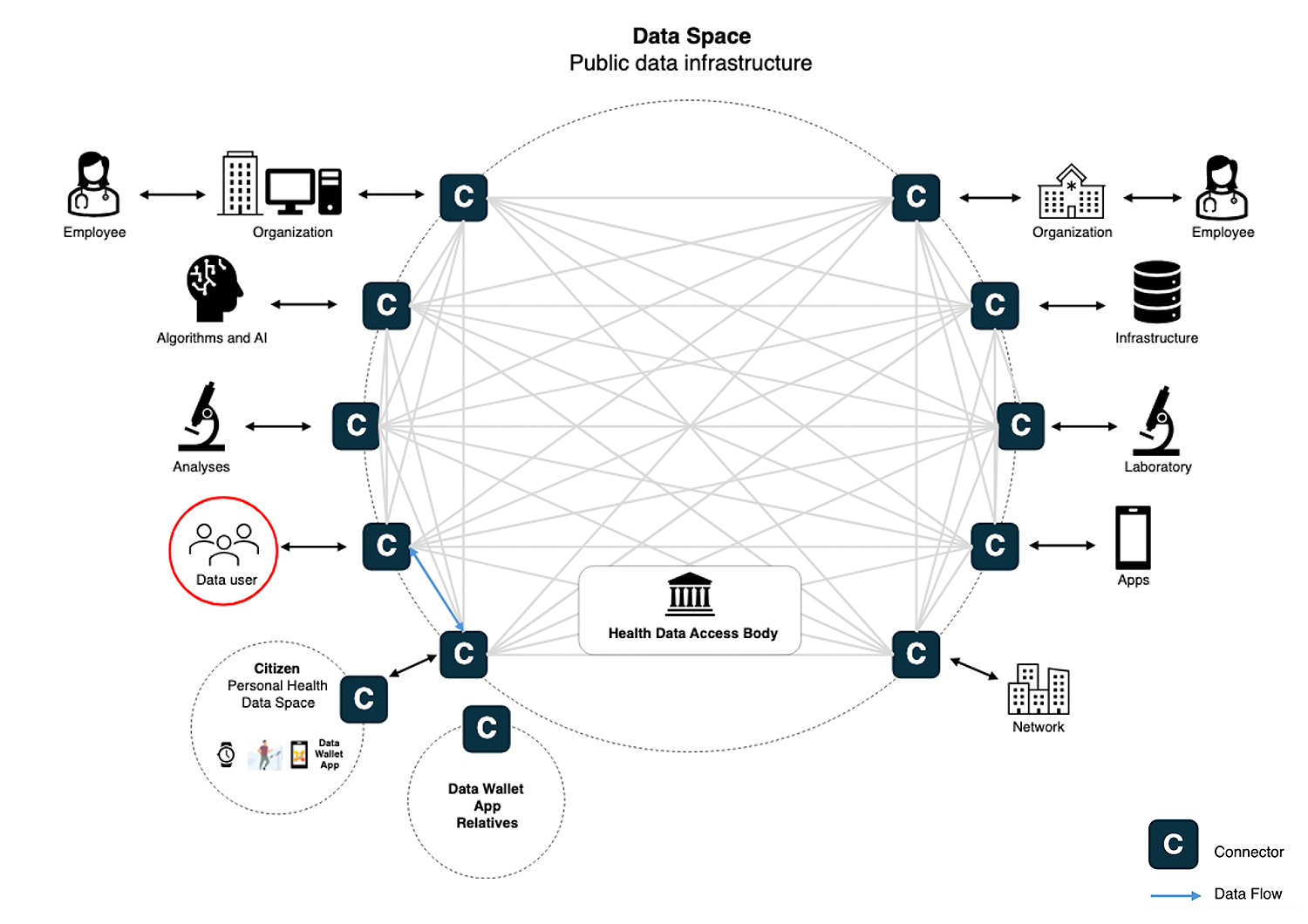
Organization-driven access pathway: Direct provision by data holders
A third pathway involves requesting data directly from data holders within existing organizational or research collaborations. In practice, you approach a data-holding organization such as a hospital, registry or research institution and request access to relevant datasets. This pathway reflects the traditional collaboration model under the GDPR, where organizations organize data sharing through contractual agreements or established research partnerships.
Within the EHDS context, such collaborations continue to play an important role. At the same time, the EHDS introduces new organizational roles and governance mechanisms, most notably Health Data Access Bodies and the possibility for certain health data holders to be designated as Trusted Health Data Holders. These actors play an important role in enabling and organizing cross-organizational access to electronic health data.
In this pathway, access is coordinated directly with the data holder. The data-holding organization prepares the dataset, performs the necessary anonymization or pseudonymization steps and ensures that data processing takes place within a secure processing environment in line with EHDS and GDPR requirements. Secure processing environments represent a central infrastructure component for analyzing sensitive health data while maintaining strong data protection safeguards (Tauscher et al., 2026). Where a data holder is designated as a Trusted Health Data Holder, it may also contribute to the assessment of access applications, while the final decision on granting data access remains with the Health Data Access Body.
For you as a data user, this pathway can enable pragmatic and flexible collaboration, particularly when trusted partnerships already exist. At the same time, you and the data holder share responsibility for governance arrangements, compliance procedures and documentation of data use. When you structure such governance arrangements, dedicated governance design tools can help clarify roles, responsibilities and access conditions within collaborative data use settings (Ugur et al., 2025).
Taken together, these pathways show that secondary data use under the EHDS can follow different organizational logics. Each pathway implies different responsibilities, coordination efforts and access conditions. When you consider these options during the exploration phase, you can better assess which pathway fits your goals, available resources and collaboration context.
Examples of health data and how they can be used
The examples below show you how different types of health data can support research, innovation and data-driven initiatives. Use them to explore which data types may be relevant for your idea and how they could connect to potential use cases. If you want to explore further, you can use the EHDS4All resources to identify additional health data sources, examples and guidance.
| Data Type | Description | Illustrative use cases |
| Clinical routine data | Generated during healthcare delivery, e.g. diagnoses, treatments, care pathways from electronic health records and clinical systems |
|
| Care and claims data | Administrative and reimbursement-related data with broad population coverage |
|
| Registry data | Structured longitudinal datasets focusing on specific diseases, interventions or outcomes |
|
| Research data | Data generated in interventional and non-interventional studies, observational research or methodological projects |
|
| Person-generated health data | Data from wearables, mobile apps or patient-reported outcomes reflecting everyday health behaviour |
|
| Imaging and sensor data | Radiological images, medical device monitoring or continuous sensor measurements requiring specialised processing |
|
| Public health and contextual data | Environmental, demographic or statistical data from open or public sources |
|
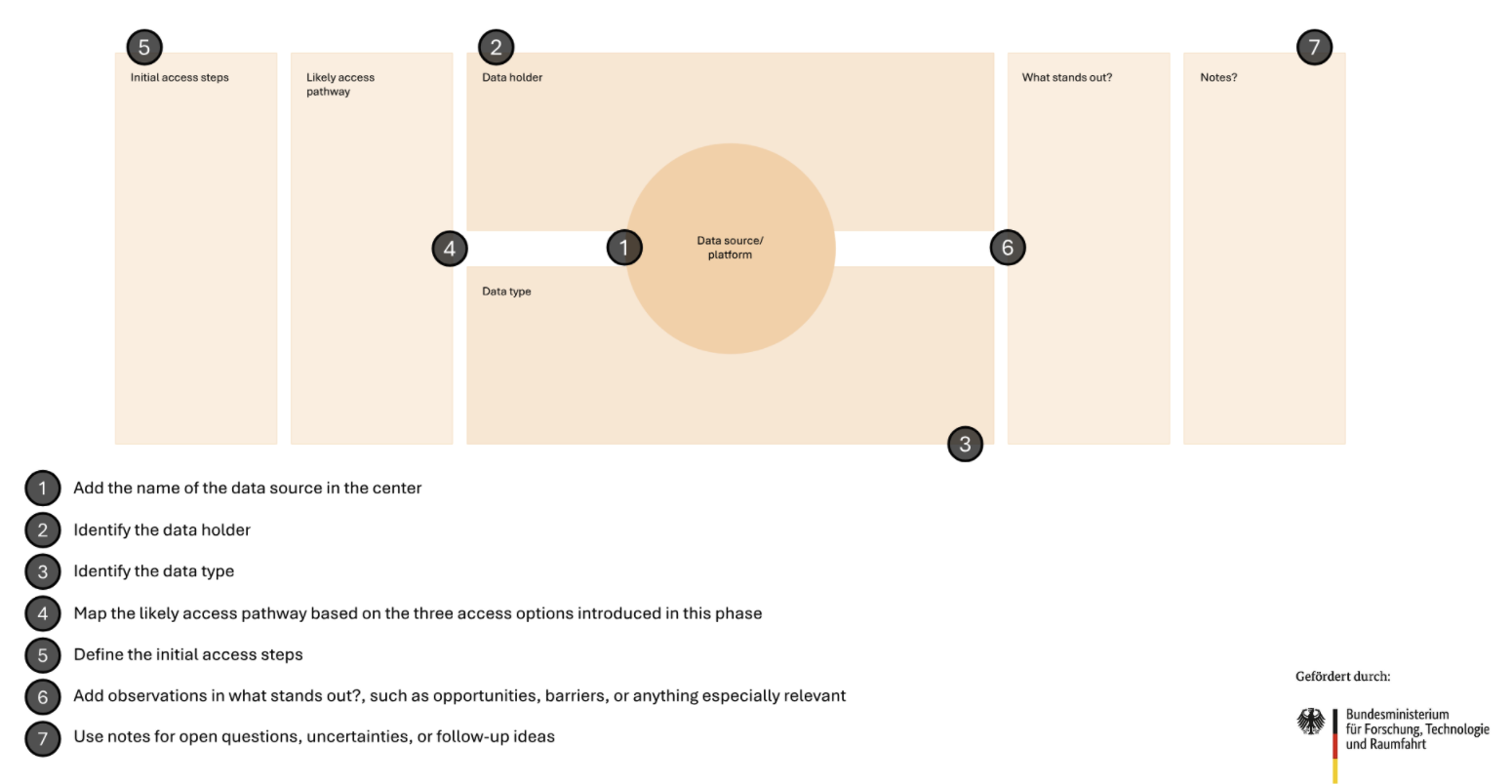
Action module: Exploring data and organizational use cases
This action module helps you explore available data and potential use cases in an open and structured way. At this stage, you focus on gaining an initial understanding of the health data landscape and reflecting on how different data sources may relate to your own objectives, challenges or areas of activity.
The data exploration canvas in the preceding section provides an overview of common health data types together with illustrative use cases. By reviewing this overview, you can familiarize yourself with the kinds of health data that exist and consider which analytical opportunities they may offer. At this stage, you do not need to assess feasibility or define concrete projects. Instead, use the table to orient yourself within the data landscape.
This module intentionally remains exploratory. You do not need to make final decisions or strategic commitments at this point. Instead, focus on developing an initial list of relevant data categories, identifying a few potential use cases or simply gaining a clearer sense of how health data could become relevant in your organizational context. In the following phases, you can then specify, prioritize and evaluate these ideas in more detail.
Data Exploration Table
Before documenting concrete use-case ideas, it may help to briefly reflect on typical scenarios in which secondary health data are used. These scenarios do not represent fixed categories. Instead, they serve as orientation points that can stimulate structured thinking.
Typical contexts include research activities such as observational studies or comparative analyses. Data may also support product development, for example in the design of digital health applications or medical technologies. Another area involves improving existing products or services, such as optimizing organizational processes or benchmarking performance. Health data can also support model development and training, for instance when developing or validating predictive algorithms. Finally, data may inform policy or system analysis, such as evaluating care structures or analyzing resource allocation.
These scenarios are not intended as strict classifications and individual ideas may overlap across several areas. Their purpose is simply to provide a frame of reference that helps you situate your reflections and recognize different possible directions of data use. You can then use the following table to document emerging ideas in a structured way.
Orienting through usage scenarios
| Usage scenario category | Examples |
| Research | Clinical studies, observation research, comparative effectiveness analysis |
| Product development | Development of digital health tools, medical devices, decision support systems |
| Product improvement | Optimisation of existing services, performance benchmarking |
| AI / Model training | Training predictive models, validation of diagnostic algorithms |
| Policy / System analysis | Evaluation of health policies, resource allocation modelling |
By completing the exploration activities, you now have an initial overview of the health data landscape and how it may relate to your organization. You have explored different types of health data, considered how they could support potential use cases and reflected on how these possibilities connect to your own objectives or challenges.
The examples and tables above help you explore possible directions of data use and identify ideas that appear particularly relevant for your context.
You can now move to the next phase of the framework. In the ideation phase, you take these early ideas and develop them further into more concrete use cases that connect organisational challenges with specific data opportunities.
Optional analytical support
If organizations already have a clearly defined intention for how data may be used, they may consult the “Methods & Analytical Tools” section to explore structured approaches for assessing data suitability. At this stage, however, such assessment is not required, as the exploration phase deliberately focuses on awareness rather than evaluation.
References
Busse, R., Blümel, M., Knieps, F., & Bärnighausen, T. (2017). Statutory health insurance in Germany: A health system shaped by 135 years of solidarity, self-governance, and competition. The Lancet, 390(10097), 882–897. https://doi.org/10.1016/S0140-6736(17)31280-1
Creswell, J. W., & Creswell, J. D. (2018). Research design: Qualitative, quantitative, and mixed methods approaches (5th ed.). Sage.
European Commission. (2025). European Health Data Space Regulation. Publications Office of the European Union.
Gliklich, R. E., Leavy, M. B., & Dreyer, N. A. (Eds.). (2020). Registries for evaluating patient outcomes: A user’s guide (3rd ed.). Agency for Healthcare Research and Quality.
Hersh, W. R., Weiner, M. G., Embi, P. J., Logan, J. R., Payne, P. R. O., Bernstam, E. V., Lehmann, H. P., Hripcsak, G., Hartzog, T. H., Cimino, J. J., Saltz, J. H., & AMIA EHR 2020 Task Force. (2013). Caveats for the use of operational electronic health record data in comparative effectiveness research. Medical Care, 51(8 Suppl. 3), S30–S37. https://doi.org/10.1097/MLR.0b013e31829b1dbd
Kahn, M. G., Callahan, T. J., Barnard, J., Bauck, A. E., Brown, J., Davidson, B. N., Estiri, H., Goerg, C., Holve, E., Johnson, S. G., Liaw, S. T., Hamilton Lopez, M., Meeker, D., Ong, T. C., Ryan, P. B., Shang, N., Weiskopf, N. G., Weng, C., Zozus, M. N., & Schilling, L. (2016). A harmonized data quality assessment terminology and framework for the secondary use of electronic health record data. eGEMs, 4(1), 1244. https://doi.org/10.13063/2327-9214.1244
Kilgus, T., Patecka, A., Schurig, T., Kari, A., Gubser, R., Gersch, M., Wessel, L., & Fürstenau, D. (2024). Creating value from the secondary use of health data: International examples, best practices, and opportunities to scale. Communications of the Association for Information Systems, 55, 507–534. https://doi.org/10.17705/1CAIS.05520
Otto, B. (2011). Organizing data governance: Findings from the telecommunications industry and consequences for large service providers. Communications of the Association for Information Systems, 29, Article 3.
Sharon, T. (2017). Self-tracking for health and the quantified self: Re-articulating autonomy, solidarity, and authenticity in an age of personalized healthcare. Philosophy & Technology, 30(1), 93–121. https://doi.org/10.1007/s13347-016-0215-5
Tauscher, F., Kari, A., & Gersch, M. (2026). From regulation to realisation: Secure processing environment for the European Health Data Space.
Ugur, F., Kari, A., & Gersch, M. (2025). Datenräume in der digitalen Pflege Entwicklung einer EHDS-konformen Architektur für sektorübergreifende Forschungsdatenkooperationen (No. 2025/10). Discussion Paper.
World Health Organization. (2021). Primary health care measurement framework and indicators: Monitoring health systems through a primary health care lens. World Health Organization.